Horner's Syndrome
What IS IT?
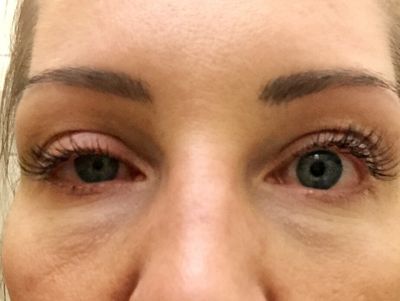
The best way to start is to clarify what is not Horner's Syndrome. Horner's Syndrome is not pink eye. According to the Genetic and Rare Diseases Information Center (GARD) website, Horner's Syndrome is a rare condition characterized by miosis (constriction of the pupil), ptosis (drooping of the upper eyelid) and anhidrosis (absence of sweating of the face).[1][2] It is caused by damage to the sympathetic nerves of the face. The presence (or lack) of anhidrosis should not be a limiting factor when ruling out Horner's Syndrome as this symptom will not present itself in internal carotid artery dissection patients due to the nerve pathways. The underlying causes of Horner's Syndrome vary greatly and may include a tumor, stroke, injury or underlying disease affecting the areas surrounding the sympathetic nerves. In rare cases, Horner's syndrome is congenital (present from birth) and may be associated with a lack of pigmentation of the iris (colored part of the eye).[1][2][3] Treatment of Horner's Syndrome depends on the underlying cause.[3]
What are the CAUSES?
There are many potential causes of Horner's Syndrome. It can be caused by any interruption in function of the sympathetic nerve fibers, which start in the hypothalamus and run via the upper spinal cord, near the carotid artery, to the face. Nerve function may be impaired due to factors such as injury, compression or a disease process. Examples of causes of Horner's syndrome include:[1][2][3][4]
- Birth trauma to the neck and shoulder.
- A stroke in the brainstem.
- Injury, blood clot or dissection of the carotid artery.
- Trauma or surgery involving the neck, upper spinal cord or chest.
- A tumor in the brainstem, hypothalamus, upper spinal cord, neck, eye, abdomen or chest cavity - particularly a neuroblastoma or a tumor of the upper part of the lung (Pancoast tumor). Neuroblastoma is one of the most common causes of Horner's Syndrome in children.
- Migraines or cluster headaches.
- Diseases that cause damage to the protective covering that surrounds nerve fibers (demyelinating diseases).
- Development of a fluid-filled cavity or cyst within the spinal cord (syringomyelia).
- Arnold-Chiari malformation.
- Inflammation or growths that affect the lymph nodes of the neck
WHAT ARE THE SYMPTOMS?
Symptoms of Horner's Syndrome typically include drooping of the upper eyelid (ptosis), constriction of the pupil (miosis), sinking of the eyeball into the face and decreased sweating on the affected side of the face (anhidrosis). These symptoms may vary and other symptoms may occur depending on the underlying cause of the condition.[1][2] Reminder: the presence (or lack) of anhidrosis should not be a limiting factor when ruling out Horner's Syndrome as this symptom will not present itself in internal carotid artery dissection patients due to the nerve pathways. Other symptoms which may be seen include the inability to completely close or open the eyelid, facial flushing, headaches and pain.[2][3]
Heterochromia iridium (i.e., a relative deficiency of pigment in the iris of affected side of the face) is usually present when the syndrome is congenital or caused by a lesion that has occurred before the age of 1-2 years of age.[3]
DIAGNOSIS
An ophthalmologist may confirm the diagnosis by special eye tests.[5] In addition, a careful neurological exam may be necessary to find the cause by determining which, if any, other parts of the nervous system are affected. Tests may include[1]:
- MRI of the head
- Carotid ultrasound
- Chest x-ray
- CT scan of the chest
- Blood tests
- Angiogram
- Eye drop tests
TREATMENTS
REFERENCES
- Horner syndrome. MedlinePlus. May 30, 2016; http://www.nlm.nih.gov/medlineplus/ency/article/000708.htm.
- Horner's syndrome. National Organization for Rare Disorders (NORD). 2003; https://rarediseases.org/rare-diseases/horners-syndrome/.
- Bardorf, CM. Horner Syndrome. Medscape. May 17, 2016; http://emedicine.medscape.com/article/1220091.
- Kedar S, Biousse V, Newman NJ. Horner syndrome. UpToDate. Waltham, MA: UpToDate; June 19, 2018; https://www.uptodate.com/contents/horner-syndrome.
- Dennis Robertson. Horner syndrome: What causes it?. MayoClinic.com. May 06, 2014; http://www.mayoclinic.org/diseases-conditions/horner-syndrome/basics/definition/con-20034650.
- Horner's Syndrome. Genetic and Rare Diseases Information Center. December 1, 2019; https://rarediseases.info.nih.gov/diseases/6670/horners-syndrome.